
Can a Shot to Prevent HIV Make a Dent in America’s Epidemic?
The long-acting PrEP medication Apretude and its backing by influential health experts hold promise, but racial disparities and a pending legal decision could hamper hopes.
By Steven Ross Johnson
Sept. 21, 2023

The recent endorsement of an injectable medication to prevent HIV transmission by a leading health task force marks a key step in efforts to end the HIV epidemic in the U.S.
At the same time, it may barely move the needle.
Cabotegravir, sold under the brand name Apretude, was backed by the U.S. Preventive Services Task Force in August as a method of preexposure prophylaxis, or PrEP, to prevent HIV transmission. The long-acting injection is taken every two months after two initial doses one month apart, and was found to lower the risk of HIV infection by 66% among men who have sex with men and transgender women compared with the use of the daily oral medication Truvada. Apretude was approved for use by the U.S. Food and Drug Administration in 2021.
The task force's recommendations encompassing Apretude trigger a requirement under the Affordable Care Act that many health insurers cover the medication without cost-sharing. For this and other reasons, the shots could change the game for some at-risk patients.
“There’s stigma associated with taking PrEP, so for people who don’t feel safe taking a medication every day, or are not able to remember to take an oral medication every day, oral PrEP is not feasible for them,” says Omar Martinez Gonzalez, senior manager of policy and advocacy for the nonprofit AIDS Foundation Chicago. “By having another option that’s long-acting that they have to take every other month, it greatly increases their ability to get on PrEP and not have to worry about taking a pill every day.”
Yet the country's disparate rates of HIV infection and preventive care, alongside varied rates of insurance coverage and a looming legal decision, threaten to counter progress that could be made and stymie efforts toward a larger goal. While the estimated number of new HIV infections among people 13 and older in the U.S. fell by 12% between 2017 and 2021, according to the Centers for Disease Control and Prevention, a much faster decline is needed to reach a government target of reducing new infections by 90% by 2030. That would mean infections would fall to around 4,000 in a year by the end of the decade.
“There’s modeling that suggests we could potentially end the HIV epidemic on the track that we are (on) in many white communities across the country, but we would not be successful in ending the epidemic in Black communities,” says Sean Bland, an assistant professor at the Santa Clara University School of Law and a scholar in health law and policy at Georgetown University’s O’Neill Institute for National and Global Health Law.
“Unless we have a strategy that not only ensures access to free or low-cost PrEP but really focuses on the geographic regions and the populations that are most vulnerable in addressing their barriers to preventable services, including PrEP, we’re not going to achieve those goals,” Bland says.
Uneven Impact
Blacks and Hispanics experience a disproportionate burden of HIV infection, with preliminary CDC data showing Black individuals accounted for approximately 40% of the 36,704 cases diagnosed in the U.S. among people 13 and older in 2022. Hispanics, who can be of any race, accounted for 31%, while whites accounted for 24%.
Yet CDC estimates also indicate only 13% of more than 468,000 Black individuals age 16 and up who may have benefited from using PrEP in 2022 were prescribed the medication. Similarly, 24% of the more than 312,000 Hispanics for whom PrEP may have been beneficial received a prescription, compared with 94% of the more than 300,000 whites in the same category.
PrEP use overall in the U.S. has steadily increased since Truvada was the first medication approved for that purpose in 2012. According to the CDC, approximately 30% of people who could benefit from PrEP were prescribed it in 2021, compared with 13% in 2017. The government’s goal is 50% coverage by 2025.
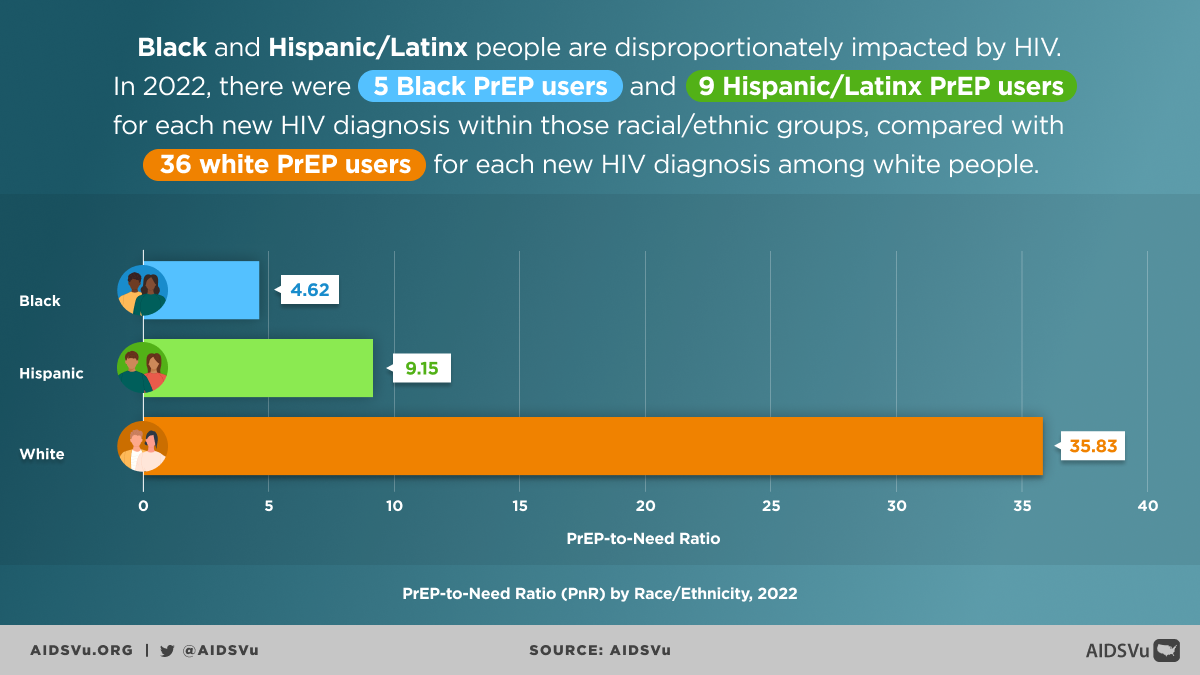
But data also indicates much of the larger increase has been fueled by higher uptake among whites, leading to growing racial and ethnic disparities. Stats from the HIV surveillance website AIDSVu – affiliated with Emory University and Gilead Sciences, which makes Truvada and the oral PrEP medication Descovy – point to approximately five Black PrEP users and nine Hispanic PrEP users for each new HIV diagnosis within those populations in 2022, compared with 36 white PrEP users for every new infection among white individuals.
{kind=link}
“Among communities of color, our sexual networks are smaller and more intertwined,” Martinez Gonzalez says. “So, if there is an outbreak of HIV within that community, then it will obviously increase the chances of coming into contact with HIV. If you also add on the layers of racial inequities in terms of access to testing, access to treatment, access to insurance and access to health care, all of that compounds together to create a crisis.”
Disparities in HIV infections and in PrEP utilization are also apparent in regional data. In the South, Black people accounted for approximately half of new HIV diagnoses in 2021 but only 21% of PrEP users in 2022, according to AIDSVu. Hispanics comprised 46% of new HIV diagnoses in the West in 2021 and accounted for only 23% of PrEP users the next year.
Dr. Laura Mintz, an assistant professor of medicine at the Case Western Reserve University School of Medicine and an internal medicine and pediatric specialist in the LGBTQI+ Pride Network of the Cleveland-based MetroHealth System, says boosting access to PrEP means making the medications more available in locations beyond LGBTQ-specialty clinics, including primary care clinics and community health centers.
But Mintz also acknowledges that having more places to access PrEP likely will not be enough to substantially increase its use in more vulnerable communities. She says several concerns, including worry over the medications’ potential costs, as well as stereotypes surrounding PrEP use, remain challenges that hinder efforts to increase uptake among people of color.
“There needs to be a couple of levers that need to be pulled for everybody to access PrEP who are eligible to access PrEP,” Mintz says.
Cost and Court Concerns
As it stands, the updated USPSTF recommendations for use of Apretude and other PrEP medications mean insurers will have to provide coverage for the drug without cost-sharing. While generic Truvada can cost around $30 a month, totaling some $360 per year, Apretude has a list price of around $3,800 per dose, according to supplier ViiV Healthcare, majority-owned by GlaxoSmithKline. That means the total out-of-pocket cost of the drug in the first year of treatment could exceed $26,000 without financial assistance. The list price of Descovy is more than $2,100 a month, according to Gilead Sciences, though insurance plans have been able to restrict its coverage in favor of generic Truvada, for example, in line with federal guidance.
But coverage for Apretude holds little benefit for the uninsured, larger proportions of whom are Black and Hispanic and for whom access to PrEP could mean paying out of pocket for at least some costs associated with the medication or the care that goes with it, such as HIV testing and injection appointments. The federal government in 2021 – following the USPSTF’s prior endorsement of Truvada – clarified that services such as HIV testing should be covered without cost-sharing by insurers as part of the PrEP process.
“Obviously for people who don’t have insurance already, this really doesn’t change anything for them,” Bland says.
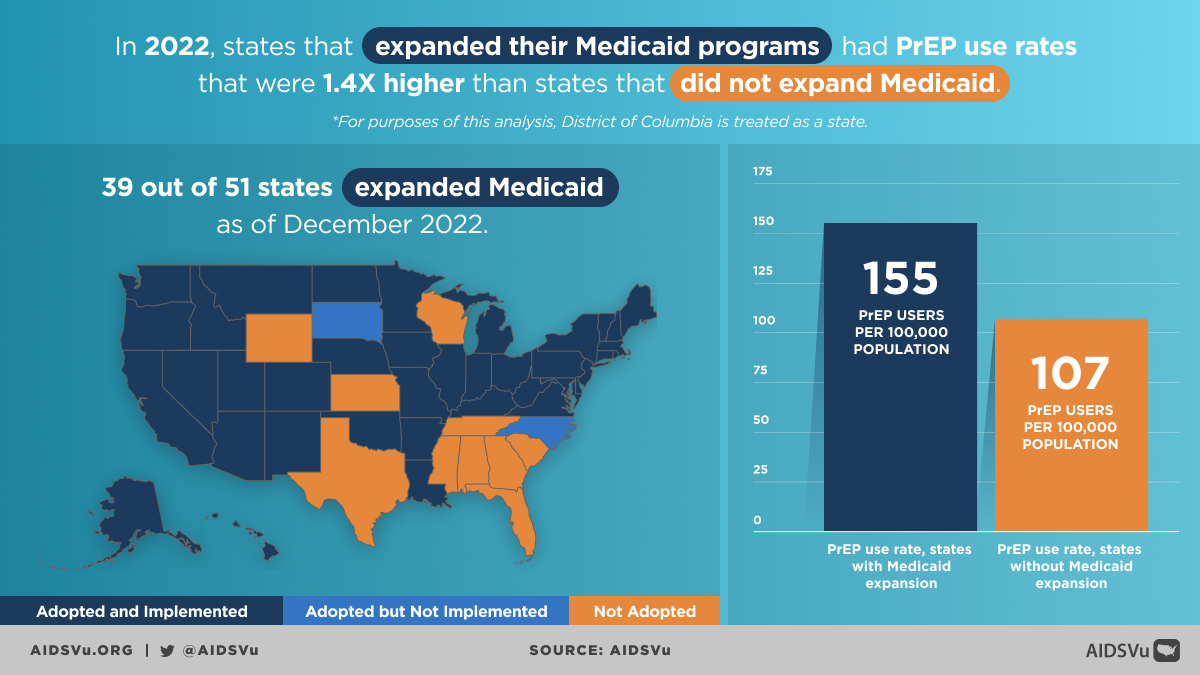
PrEP drugmakers offer financial aid programs, as do at least some states and the federal government through the no-cost, oral medication-focused Ready, Set PrEP program. Still, authors of a recent analysis of uncovered costs associated with PrEP noted that policies promoting health insurance access, such as Medicaid expansion, could improve access. According to AIDSVu, states that had expanded Medicaid posted rates of PrEP use in 2022 that were 1.4 times higher than states that had not.
{kind=link}
Meanwhile, a pending ruling in a federal appellate court looms as a threat that could more broadly undermine PrEP coverage. In March, a district court judge in Texas struck down part of the ACA requirement for no-cost coverage of preventive services recommended by the USPSTF, along with finding that requiring coverage for PrEP violated the religious rights of specific plaintiffs who sued.
The decision has largely been put on hold pending review by the 5th U.S. Circuit Court of Appeals, which could rule on the case this year. An expansive ruling – one not tailored just to the plaintiffs – could gut the preventive services mandate in relation to at least some care, such as PrEP. And Laurie Sobel, an associate director for women’s health policy at research and polling organization KFF, says the government could be forced to seek an emergency stay until the case could be appealed to the U.S. Supreme Court.
“It’s an open question about how broad that (ruling) could be at the 5th Circuit or at the Supreme Court,” Sobel says. “We don’t know what the 5th Circuit could do.”
In the wake of the March court ruling, insurers expressed support for preventive services. Still, Lindsey Dawson, associate director of HIV policy and director of LGBTQ health policy for KFF, says there is little doubt a decision against the preventive services mandate could have broad health implications.
“Right now, PrEP uptake is quite good among gay white men, but among people of color and among women PrEP access is quite limited,” Dawson says. “Taking a tool out of the toolbox with the elimination of access to no-cost PrEP through insurance could jeopardize that further.”
Changing the Narrative
Torrian Baskerville, director of HIV and health equity for LGBTQ+ advocacy organization the Human Rights Campaign, says a big challenge in trying to increase PrEP use in underserved communities has been a lack of awareness among both individuals who would benefit from using it and among the clinicians that provide their care.
Baskerville says there is a general shortage of clinicians outside the network of LGBTQ-specific health care providers who have the skills and experience to identify patients who could benefit from PrEP and offer it to them.
“Many times, individuals go to their health care provider and ask for PrEP, and because their primary care physician is not knowledgeable, they choose not to provide it,” Baskerville says.
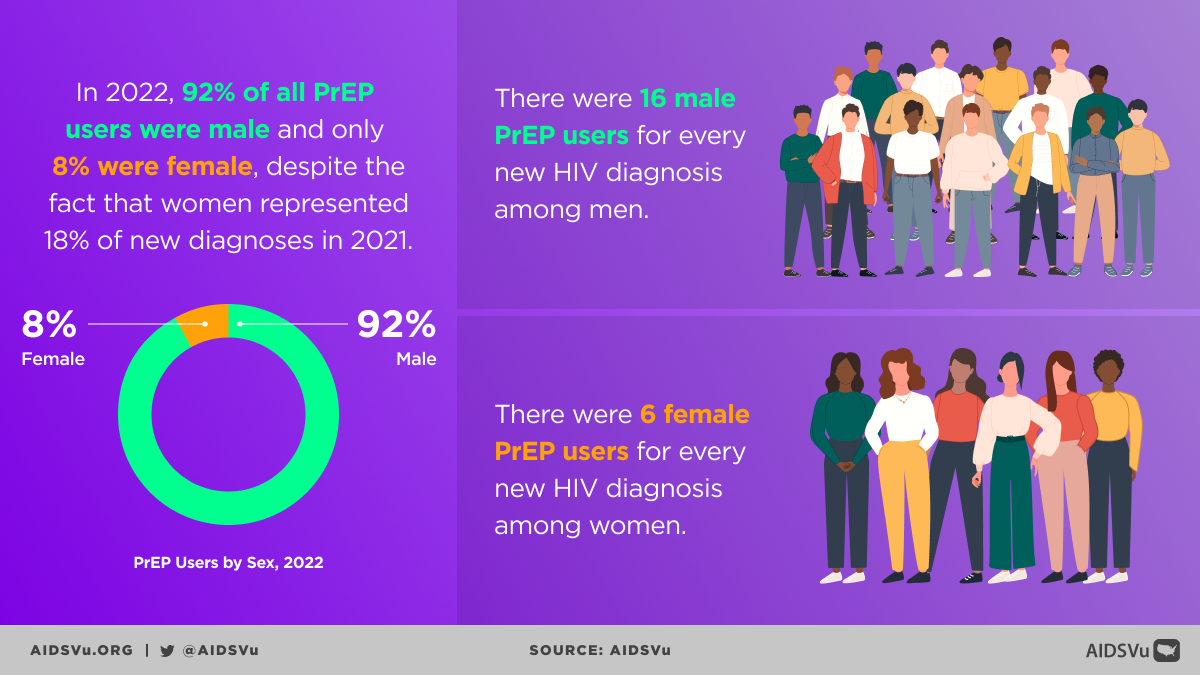
Preconceived notions that PrEP is only for LGBTQ individuals can be a hurdle to others receiving it who still may benefit. According to CDC estimates, 70% of new HIV infections in 2021 were among men who’d had sexual contact with other men, but 16% occurred among women who reported heterosexual contact. Women accounted for only 8% of PrEP users in 2022, according to AIDSVu.
{kind=link}
“I do think that the notion that PrEP is only for gay men and trans women rather than all of the people who would be eligible for PrEP is another thing that impairs the power of PrEP to end the HIV epidemic,” says Mintz, of the MetroHealth System in Ohio. “There are a ton of people who could be offered PrEP who are having multiple sexual partners, or (who are) with someone who has multiple sexual partners whose HIV risk could be reduced substantially.
“Homosexual, heterosexual or bisexual – whatever kind of activity people are having, all of those people should be offered PrEP as an opportunity to prevent HIV.”
Attempting to fill the information gaps about PrEP has been a major objective of MetroHealth’s PrEP navigator program, which has led the health system’s outreach to predominantly racial and ethnic minority communities of late. Navigators have visited communal places like nightclubs to talk with people about the potential benefits of the medication.
Mintz says clinicians also need to include talking about access to PrEP as a routine part of their review of a patient’s sexual history and practices to help reduce stigma around the medication.
“It should be discussed as regularly as birth control,” Mintz says.
Next Steps
Baskerville and others feel a robust national strategy for distributing PrEP is needed to provide the medication to the most impacted communities at little to no cost. Yet the current political landscape makes the likelihood of enough federal funding to that end unlikely.
As part of his fiscal year 2024 budget request to Congress, for example, the Biden administration in March proposed allocating $850 million for the government’s Ending the HIV Epidemic in the U.S. initiative, according to KFF, as well as $9.8 billion over the next 10 years for a mandatory PrEP program that would cover the cost of the medication for uninsured and underinsured people.
Notably, the EHE effort has aimed to initially focus on more than 50 geographic areas that have been hit particularly hard by HIV. And the mandatory PrEP program “would include PrEP drugs, associated lab services, and ancillary services to support PrEP uptake and consistent use by clients,” according to a Department of Health and Human Services budget document.
In July, however, Republicans in the House of Representatives released a proposed fiscal year 2024 appropriations budget that reportedly seeks to cut CDC funding by $1.6 billion and zero out funding for the agency’s share of the EHE initiative.
Regardless of whether a national PrEP program would be implemented, Bland says the success of any effort to end the HIV epidemic for all populations in the U.S. will depend on how well it focuses on eliminating access barriers to preventive services in areas where HIV infection rates among Black and Hispanic individuals are at their highest.
“We need to make sure we are maintaining a focus on the populations in the geographic regions where we’re seeing the infections and ensuring that we’re funding community-based organizations and clinics that serve those populations in the ways that they need,” Bland says.
